The primary goal of antimicrobial susceptibility testing (AST) in a clinical setting is to assist veterinarians in optimal antimicrobial selection for their case. This may be done as part of individual patient management or applied to a population, like a herd or flock. Outside of individual case management, AST is used for antibiogram development to guide empiric therapy and surveillance and monitoring programs contributing to our understanding of how bacterial populations vary regionally and change over time.
What is AST?
AST evaluates inhibition of bacterial growth after exposure to an antimicrobial drug in a liquid media or on an agar plate.
How is AST performed?
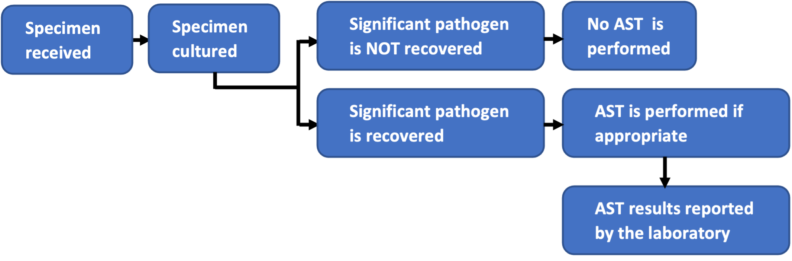
It is important to remember that an appropriate specimen from an animal with a suspected bacterial infection is essential to accurate test results. The general in-laboratory AST workflow includes:
Testing can be divided into diffusion-based and dilution-based methods. In both cases, live bacteria must first be isolated and identified through culture methods.
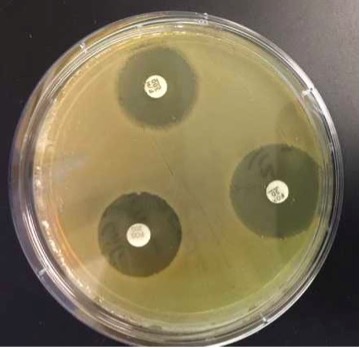
Diffusion Method
A known concentration of bacteria are exposed to antimicrobial-impregnated disk which diffuses through the agar at a predictable distance. The size or location of the inhibitory zone (aka: zone diameter) is measured in millimeters and is unique for each drug/bacteria combination. Examples: Kirby-Bauer disk diffusion, Etest® gradient strip method.
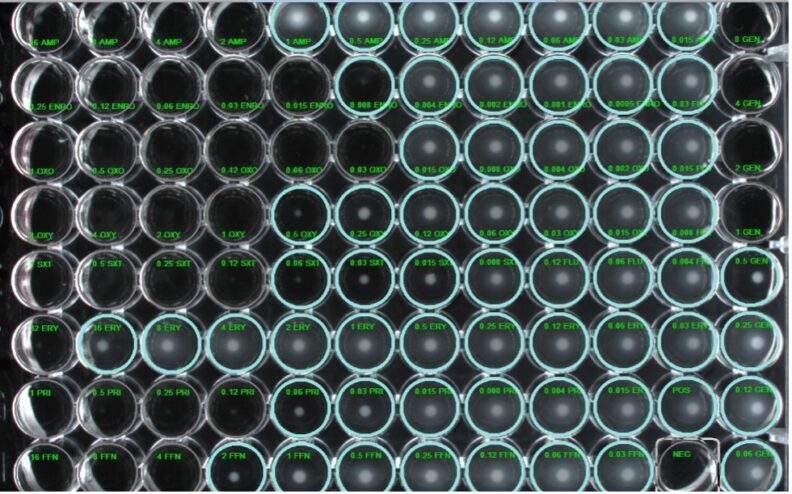
Dilution-based
Dilution based methods are performed by incubating a known concentration of bacteria with serial two-fold dilutions of antimicrobial drug. This can be performed in a semi-automated system with microtiter plates, in test tubes, or in agar. At WADDL we perform broth microdilution. The lowest concentration without visible bacterial growth is the minimum inhibitory concentration (MIC) and is usually reported as mg/ml.
What can impact the quality of AST?
Confidence in the accuracy of any laboratory results is directly related to quality control, and AST is no exception. Starting with a quality specimen is key to isolating only those bacterial species that are involved in the disease process. Contamination by environmental or commensal bacteria will limit the utility of AST.
Deviations in laboratory protocols may lead to erroneous AST results. For example, in disk-diffusion, the agar thickness can impact the diffusion of the antimicrobial agent. In broth microdilution, loading microtiter plates with too much or too little inoculum can lead to a resistant bacterium being called susceptible or vice versa. Following standardized procedures is crucial to accurately perform AST.
How are AST results reported?
The AST results are reported as susceptible, susceptible dose-dependent, intermediate, and resistant using clinical breakpoints to interpret minimum inhibitory concentration (MIC) or zone diameter data obtained from in vitro testing. These interpretive categories are defined:
- Susceptible (S) – isolates with an MIC at or below (or a zone diameter at or above) the susceptible breakpoint are inhibited by the usually achievable concentrations of antimicrobial agent when the dosage recommended to treat the site of infection is used, resulting in likely clinical efficacy.
- Susceptible dose-dependent (SDD): isolates with an MIC at the SDD breakpoint require a dosing regimen that achieves higher drug exposure which is different then the regimen used to set the susceptible breakpoint.
- Intermediate (I) – isolates with MICs (or zone diameters) within the intermediate range that approach usually attainable blood and tissue levels and for which response rates may be lower than for susceptible isolates; NOTE: The intermediate category implies clinical efficacy in body sites where the drugs are physiologically concentrated or when a higher-than-normal dosage of a drug can be used. Additionally, this category accounts for lab technical variability.
- Resistant (R) – isolates with an MIC at or above (or a zone diameter at or below) the resistant breakpoint are not inhibited by the usually achievable concentrations of the agent with normal dosage schedules and/or that demonstrate MICs that fall in the range in which specific microbial resistance mechanisms are likely, and clinical efficacy of the agent against the isolate has not been reliably shown in isolates with similar phenotypes.
What is a breakpoint and how is it determined?
Breakpoints are established by the Clinical and Laboratory Standards Institute (CLSI) to predict clinical outcomes. A “susceptible” isolate predicts a likely clinical success using the dose, route and frequency of administration used to develop the breakpoint. A “resistant” isolate predicts a low probability of success following treatment.
Breakpoints are developed by the CLSI through evaluating:
- Concentrations of drug needed to inhibit growth of bacteria with no acquired resistance (pharmacodynamics)
- Achievable plasma drug concetrations in the animal (pharmacokinetics)
- Knowledge of drug properties (concentration vs time-dependent, protein binding)
- Clinical outcome trials.
They may be developed for individual bacterial species, genera or bacterial families and are specific for an animal species. Some may be specific for an anatomical site. All breakpoints are developed using one antimicrobial dosing regimen (dose, route, frequency of administration). In situations where antimicrobial treatment regimens deviate from the clinical breakpoint dosing regimen (ie: increased dose, different route of administration, etc.), AST interpretation may not be as predictive.
What does the lab do if no breakpoints exist?
Successful antimicrobial therapy relies on the antimicrobial agent reaching the site of infection at a concentration that inhibits growth or kills bacteria. Much of the ability of a drug to reach a site is animal species specific and the concentration needed at the site must be relevant to a specific bacterial species. For example, cefovecin can be highly bound to plasma proteins with considerable animal species variability, therefore the cefovecin breakpoints of dogs and cats should not be used for other animal species. Thus, breakpoints developed for one animal species, bacterial group or anatomical site may be inappropriate to be used for a different species of animal, bacteria or anatomical site. Extrapolation must be made with caution to not over-estimate efficacy of therapy.
Common extrapolations may be:
- Canine breakpoints used for feline infections
- Bovine breakpoints used for small ruminant infections
- • Equine skin/soft tissue breakpoints used for respiratory infections
Often human specific breakpoints are used to interpret AST results due to lack of any veterinary-specific information. While these breakpoints may indicate resistance (generally align with mutational resistance detection) the clinician should be aware that the susceptibility interpretation may not confidently apply to their case due to large differences in pharmacokinetics. Ideally, laboratories should indicate what breakpoints were applied if alternatives are used.
Many knowledge gaps still exist in veterinary-specific resistance breakpoints and extrapolations are not uncommon. It is important to be aware of this situation and to evaluate AST data accordingly. Further research in animal-specific breakpoints is urgently needed.
Should I choose the antimicrobial agent with the lowest MIC on my report?
No. The PK/PD of the antimicrobial will be different for individual drugs which changes the range of dilutions tested to account for this difference.
One of the laboratories I submit samples to reports more antimicrobials than another. Am I receiving more value from my submission to have more antimicrobials reported?
Not necessarily.
When labs perform a broth microdilution AST, a panel of antimicrobials are being evaluated. The antimicrobials included are dependent on the manufactured commercial plate. Typically, a panel of approximately 20-24 antimicrobials are evaluated. The commercial plates have been developed to test antimicrobials with dilution ranges that reflect the PK of antimicrobials within an individual species. While some labs choose to report the entirety of the panel evaluated, other labs will selectively report only those antimicrobials that could be useful for the case. If the entirety of the panel is reported, the prescribing veterinarian must understand the factors that would limit the use of a particular antimicrobial for their patient, and what antimicrobial AST results can be used to predict activity of other antimicrobials not directly tested. Labs reporting only those antimicrobials that have an effect against the identified bacterial isolate have done this work for the submitter.
Why does the AST report say the isolate is susceptible, but the patient is not responding to treatment?
Many factors account for successful treatment outcomes beyond susceptibility of the bacteria to antimicrobials. Disease effects such as chronicity of the disease process or presence of other infectious agents may decrease antimicrobial therapy response. Antimicrobial tissue penetration may be reduced by decreased blood flow as in shock or in abscesses. Infection of protected sites like the central nervous system or prostate gland may preclude antimicrobial activity due to poor tissue penetration. Other local effects may prevent antimicrobial effectiveness such as biofilm in a surgical implant, cellular debris like pus and necrotic tissue, local pH, and oxygen concentrations. Compromised organ function of the patient can affect the target site antimicrobial concentration. The immune status of the patient also plays a significant and often overlooked component of a therapeutic success. All these factors are not assessed through AST and can affect the outcome for the patient.
Why is the patient responding to treatment when the AST report says the isolate is resistant?
Many veterinarians will have marveled how animals can have successful treatment outcomes despite lack of therapeutic intervention. For individual cases a specific bacterial isolate may have resistant AST results, however a patient’s immune system has amounted a robust response and antimicrobial therapy was not a factor in the treatment outcome. This can be common when foreign material or underlying factors are corrected, aka “source control”. Secondly, the significance of the bacteria isolated may be over interpreted and we are dealing with colonization and not infection. Finally, antimicrobial therapy may be targeting an bacterial species not recovered on culture that is clinically relevant. This is not an exhaustive list.
Why is AST not performed on all bacterial growth from a culture?
Bacterial isolates must first be cultured and identified and clinical significance determined. Depending on the source of the specimen, environmental or commensal bacteria may be cultured. Deciding which bacteria in mixed growth are significant, especially within the presence of commensal bacteria (ie: skin, vaginal or gastrointestinal microflora), can be difficult. Performing AST on all isolates can overemphasize the importance of the bacteria as they may be normally present at the site or reflect contamination rather than be involved in the disease process. Communication with the laboratory regarding interpretation of culture growth is highly encouraged when these issues arise.
Should AST be performed in all cases prior to antimicrobial therapy?
Much consideration needs to be given to the presenting case in choosing what diagnostic testing to pursue prior to treatment decision making. Factors such as severity and chronicity of the condition, age of the patient, likelihood of deterioration, and cost of care may preclude having AST results prior to initiating antimicrobial therapy. Empiric selection of an antimicrobial based on the clinician’s experience and judgement of the likelihood of a specific bacterial infection can be more prudent than collecting a specimen and waiting for bacterial isolation and AST. Prudent antimicrobial use does not mean withholding antimicrobials from a patient who would benefit from therapy while awaiting AST results. In certain cases, bacterial identification is more useful for guiding therapeutic decisions and AST is unnecessary, for example isolation of β-hemolytic Streptococci. In cases that have failed to respond to empiric therapy, bacterial culture and AST is likely necessary to guide further antimicrobial selection. This can be especially important in cases involving bacterial species known to have acquired antimicrobial resistance (i.e.: Staphylococci, Enterobacterales, Enterococci, Pseudomonas aeruginosa) and requires AST to assess the resistance profile of the isolate.
Should AST be performed during antimicrobial therapy?
In general, collecting a specimen from an animal being treated with antimicrobials should be avoided. Residual antimicrobial compounds can inhibit bacterial growth of a clinically relevant organism. However, if therapeutic failure is observed culture may be indicated. Depending on the case, a wash-out period of 3-4 days will reduce the effect of a previously administered antimicrobial on AST. If the patient has been on antimicrobial therapy, including this information as part of the specimen submission can improve case interpretation from a clinical veterinary microbiologist.
Can the results of an AST be used to predict outcomes in other cases?
In a herd or flock setting, monitoring AST profiles of commonly isolated bacteria can be useful in assessing susceptibility pattern shifts in the population. Regionally, labs can collate AST data and present a cumulative antibiogram, summarizing the susceptibility profiles of a particular bacterial species in the form of percentage susceptible to a specific antimicrobial compound. Both of these circumstances use previous AST results to predict susceptibility patterns of bacterial species in a given population and provides a reasonable basis for empiric therapy. When empiric therapy fails for an individualized patient evaluation of the specific AST profile of a clinically relevant bacterial isolate can be very important for targeted antimicrobial selection.
Where can I find more information about AST and its interpretation?
Excellent resources outline the procedures, utility, and limitations of AST testing:
- CLSI. VET09: Understanding Susceptibility Test Data as a Component of Antimicrobial Stewardship in Veterinary Settings. 2nd ed. CLSI report VET09. Wayne, PA: Clinical and Laboratory Standards Institute; 2019.
- CLSI. VET01S: Performance Standards for Antimicrobial Disk and Dilution Susceptibility Test for Bacteria Isolated from Animals. 7th ed. Wayne, PA: Clinical and Laboratory Standards Institute; 2024.
- Clinical and Laboratory Standards Institute (CLSI) free resources
- Giguère S, Prescott JF and Dowling PM. Antimicrobial Therapy in Veterinary Medicine. 5th ed. Ames, IA: Wiley Blackwell; 2013.